[ad_1]

Australia has one of the world’s highest levels of ultraviolet radiation, a proven carcinogen that causes skin care and eye diseases. UV damage is said to accumulate from childhood, and the risk of developing UV-associated diseases increases with age.
Reportedly, one Australian is diagnosed with melanoma every 30 minutes, while 50 people are diagnosed with UV-related cataracts daily. Early detection is greatly emphasised to identify people at high risk of getting UV-related diseases. Current solutions include a questionnaire for recording sun-safe behaviour and UV-sensing wearable devices that only measure an individual’s daily or monthly UV exposure levels.
Another solution is a desktop system for assessing the damage caused by UV radiation exposure to the eye. A new study in Australia now aims to translate this into a mobile system for routine skin cancer screening.
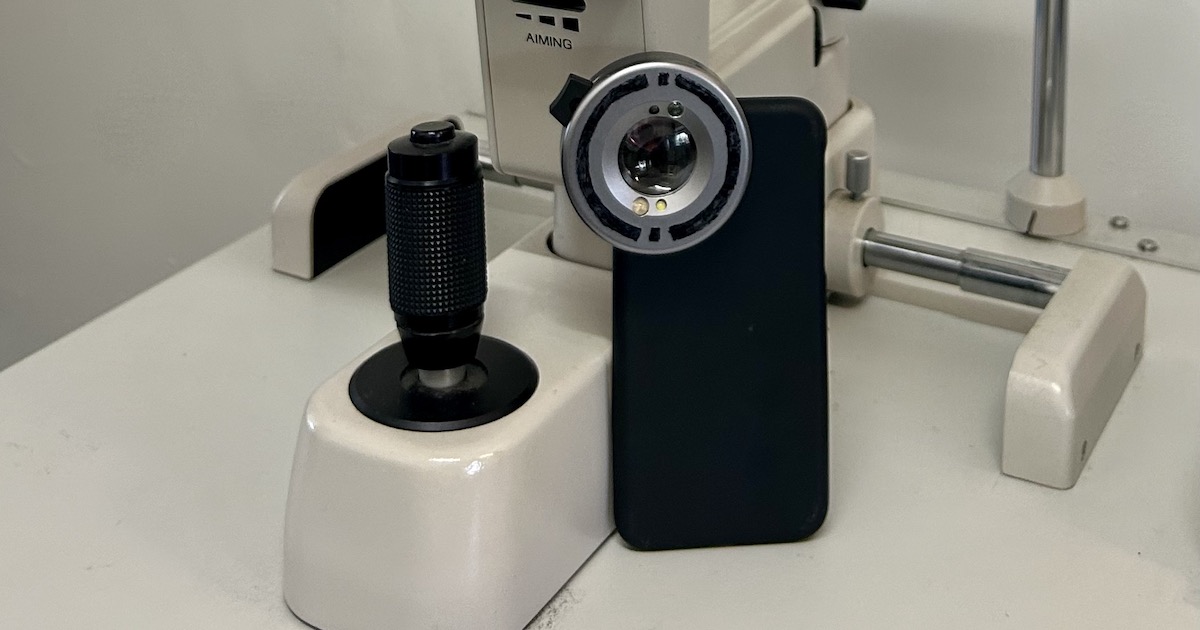
It involves a UV light camera attached to a smartphone camera to capture eye images for conjunctival UV autofluorescence (CUVAF), a method of measuring the damage to the conjunctiva due to UV exposure. A companion mobile application then analyses the images to calculate the UV damage to the eye.
Minas Coroneo, a professor at the Department of Ophthalmology in Prince of Wales Hospital who is leading this research, has done pioneering work that documented how UV-related diseases, such as pterygium (tissue growth on the cornea), can be an early indicator of skin cancer, decades before its onset. His team was behind the desktop-based UV damage assessment system, which features a benchtop camera and software. He is now working with other professors from the University of Technology Sydney (UTS) and the University of Western Australia (UWA) to adapt this system to smartphones, supported by an A$125,000 grant from the Prince of Wales Hospital Foundation.
Prof Coroneo further discussed with Mobihealth News how their screening method works and how the assessment of UV damage to the eye can be incorporated into preventative health.
Q. Can you explain how the existing desktop CUVAF device works?
A. Both desktop and portable devices work on the principle of UV fluorescence photography, a well-established method we adapted from dermatology in ~ 2005. UV light is used to illuminate the body. It interacts with the skin and is reflected at a longer wavelength than used in illumination. These spots were thought to represent damage to collagen in the skin. We took this method and adapted it for use in the eye.
Together with UWA professor David Mackey, we first created a portable system that he used in epidemiological studies in places like Norfolk Island. We also worked out a way of quantifying the area of fluorescence and its brightness.
Along the way, we thought about a smartphone system – Chinese and Indian systems became available but none of them took off. They have also been validated against a system like our desktop system.
I started collaborating with Mojtaba Golzan, an associate professor at UTS, on a different project. He has built the prototype we are currently using and is working on.
Q. How did your team figure out UV-related ocular damage as an early sign of skin cancer?
A. The link is by inference. Pterygium is associated with skin cancer, including melanoma; early evidence of ocular UV damage is a predictor of pterygium development and pterygium is associated with later development of skin cancer.
Q. When did you come up with the idea of developing a mobile prototype of the CUVAF? Can you walk us through the process of adapting its mechanisms (software or algorithm, UV camera capture) to a smartphone?
A. The first work with Prof Mackey was published in 2011. We made a portable version of the desktop camera system so it could be carted all over Norfolk Island. From that time, we were actively trying to further miniaturise the system, mostly from a field testing perspective. 2011 smart cameras were not up to the task, neither were small UV lighting systems. As these further developed, we tried different generations of mostly iPhones. It was not until the more recent smartphones with better cameras – and the collaboration with A/Prof Golzan – that progress was made.
We repurposed smartphone clip-on devices for taking close-up shots, including of the eye. A/Prof Golzan has used AI trained on the real-world data we have generated with the [camera add-on] to calculate fluorescence hot spot areas and brightness. The algorithms developed by Prof Mackey have been optimised for the desktop system. While they could be adapted to the new device, we believe the AI system will be faster and as accurate.
Q. Can smartphone-based UV damage assessment be incorporated into daily personal care management?
A. Our aim is to assess the suitability of smartphone-based UV damage assessment in children. Doing daily assessments would be overkill since changes likely occur over long periods of time. Much of the [UV] damage may occur during the summer months and repairs happen during winter. We do not know the ideal level of UV exposure; after all, UV exposure still has some benefits, such as vitamin D production and countering myopia development. I think a seasonal self-assessment would be adequate.
Q. To what extent can health professionals/health providers and consumers rely on smartphone technology for preventative healthcare?
A. This will depend on validated and adequately trialled systems. We believe we are in good shape to validate our smartphone device against the system we first developed and which has the longest and largest track record of any such device.
There are concerns that [eye and skin protection messages] are not getting through adequately; telling kids to wear sunglasses and a hat may not be as powerful as empowering them to see damage to their own eyes and following the extent of damage through the seasons and over the years.
_
Prof Coroneo’s answers have been edited for the sake of brevity and accuracy.
[ad_2]